
History
Hugo is a 17 year old Warmblood gelding used for show jumping. Hugo had a 12 month history of acute onset grade 3/5 left hind limb lameness. Hugo was diagnosed with proximal suspensory desmopathy in the left hind and rested for 12 months with failure to improve. The gelding was reevaluated recently and was positive to upper limb flexions and the lameness improved 90% to a deep branch lateral plantar nerve block. Radiographs taken at this time revealed left hind distal hock osteoarthritis and unusual lucencies of the distal tarsal bones. Ultrasound of the area revealed enlargement of the proximal suspensory ligament. Hugo was referred to Animal Imaging for the use of the 3T magnet to evaluate the origin of the suspensory ligament and distal tarsus.
Image Findings
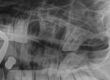
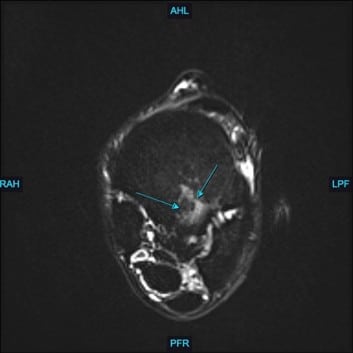
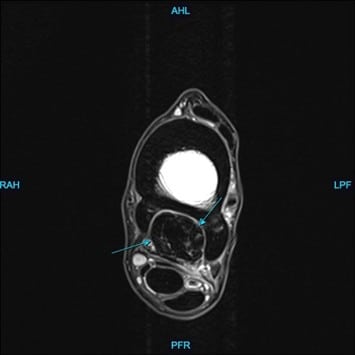
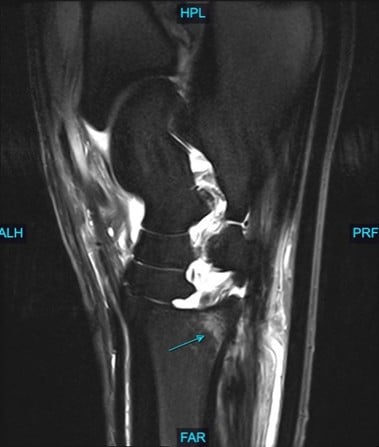
At Animal Imaging, Hugo was placed under general anesthesia and multiplanar MR images were acquired. The gelding was found to have moderate to marked, ill-defined fiber disruption of the origin of the proximal suspensory ligament with marked subchondral and endosteal sclerosis of proximal plantar third metatarsal. The proximal and body of the suspensory ligament was generally enlarged and rounded. The gelding also had marked subchondral sclerosis of dorsal central and third tarsal bones. Numerous, small cortical and subchondral cystic lesions of the dorsal distal intertarsal and tarsometatarsal joints.
Conclusion
Hugo was diagnosed with subchondral bone injury of third metatarsal bone with concurrent marked enthesitis and desmopathy of the origin of the proximal suspensory ligament. The gelding also had moderate to marked chronic desmopathy of the proximal suspensory ligament and body and Moderate to marked distal intertarsal and tarsometatarsal osteoarthropathy.
Proximal suspensory desmitis in the hindlimbs of performance horses is not uncommon. This injury occurs when the ligament is stretched beyond its capabilities which can be caused by multiple factors including upright hindlimb conformation, stress-induced injury, uneven footing, or underlying pathology. Most commonly this injury occurs from cumulative damage rather than one traumatic event. Due to the location of this ligament between metatarsals two and three, the swelling that occurs places pressure on the lateral plantar nerve which causes discomfort to the horse. Many different options for treatment exist, including rest, shockwave, intra-lesional injection, and even surgical approaches of fasciotomy of the proximal suspensory ligament combined with neurectomy of the deep branch of the lateral plantar nerve.