
History
Marty, a 5 year old male neutered Labrador Retriever, was brought to the emergency room after Marty became painful and started to limp. There was no traumatic event the owners could recall and the examination at the emergency room found nothing of significance. Marty had shockwave therapy, chiropractic work, acupuncture, and Adequan to improve the discomfort but there was no improvement. Radiographs were taken which revealed mild arthritis and some laxity in the left hip. 2 months after the initial trip to the ER, Marty began sliding both feet forward while in a sitting position as well as unwillingness to jump on to things. Marty’s discomfort revolved from lumbar pain, to cervical pain, to hip pain and Marty was referred to Animal Imaging for an MRI to look for a cause for his clinical signs. Pre-anesthetic bloodwork was normal except for an increase in globulin of 4.2 g/dL (rr 1.6-3.6 g/dL).
Imaging Findings
At Animal Imaging, Marty was placed under general anesthesia and multiplanar MR images were acquired before and after intravenous contrast. No abnormalities of the cervical spine were identified, including no evidence of spinal cord compression or intramedullary lesions. In the thoracic spine, a few of the thoracic intervertebral discs have reduced signal on T2 images, consistent with desiccation/degeneration but there was no evidence of thoracic spinal cord compression or intramedullary lesions are identified.
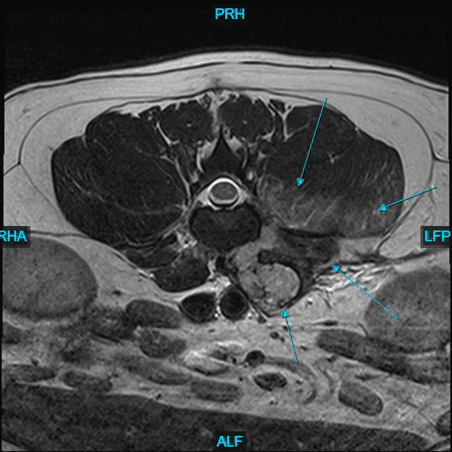
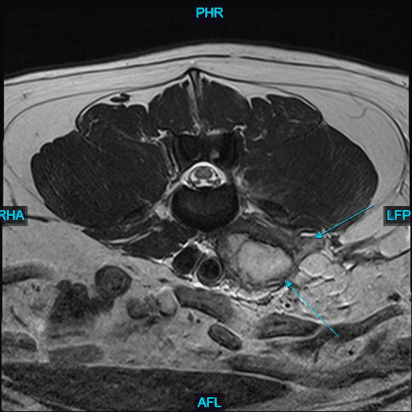
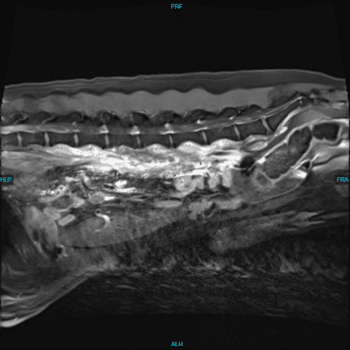
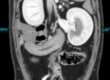
However, in the lumbar section of the spine, along with a few mildly protruding discs, there was a large, irregularly marginated accumulation of T2/STIR hyperintense fluid and/or necrotic tissue present in the iliopsoas muscles near midline at L1 and primarily within the diffusely enlarged left iliopsoas musculature from L2 to L6. This fluid and enlarged left iliopsoas muscle was causing ventral deviation and bulging of the dorsal peritoneum. In addition to this tissue, there was also 1 to 2 mildly enlarged lymph within the caudodorsal and mid abdomen.
Discussion
Large paravertebral accumulation of fluid and/or necrotic tissue with adjacent contrast-enhancing musculature along the ventral lumbar spine (left> right), with probable involvement/inflammation within the left retroperitoneal space. The primary differentials include a muscle injury/tear with a hematoma (e.g., secondary to trauma) vs a paravertebral abscess (e.g., secondary to a migrating foreign body or hematogenous infection) with adjacent myositis/cellulitis. Neoplasia is also possible but felt less likely.
Conservative management was elected and routine ultrasonographic examinations showed little change in the appearance of the accumulation but a 30 day course of antibiotics with rehabilitation therapy including acupuncture, underwater treadmill, and herbal supplements improved Marty’s clinical signs.