
History
An eight year old Quarter Horse gelding used for reined cow horse work was referred to Animal Imaging for a 3T MRI of the left hind distal limb. At the end of July, the horse was grade 4/5 lame and blocked to an abaxial nerve block. There were no significant findings on radiographs. He was given stall rest and NSAID therapy. Twelve days later, the horse was grade 2/5 lame in the left hind and the coffin joint and tendon sheath were injected at that time (medication not specified). One week later, the horse was grade 3/5 lame in the left hind. The fetlock and tendon sheath were blocked, but there was no resolution of the lameness; however, he did block sound to a lateral abaxial nerve block. Two weeks afterwards, the horse was grade 2/5 lame in the left hind and blocked 80% to a lateral abaxial nerve block and was 100% sound after the medial abaxial nerve block was placed. Radiographs were repeated along with an ultrasound exam with no significant findings. Throughout the 6 week history of lameness, the horse would improve with rest and NSAID therapy, but would become more lame as the workload was increased.
Clinical Exam Findings
Upon presentation to Animal Imaging, all physiological parameters were within normal limits. Hoof testers were mildly positive in the left hind foot. In hand on a hard surface, the horse was grade 2/5 lame in the left hind. He was moderately resistant to flexion of the left hind distal limb. A mild amount of soft tissue swelling was noted distally in the left hind.
Imaging Findings: Left Hind Foot
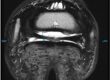
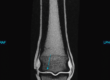
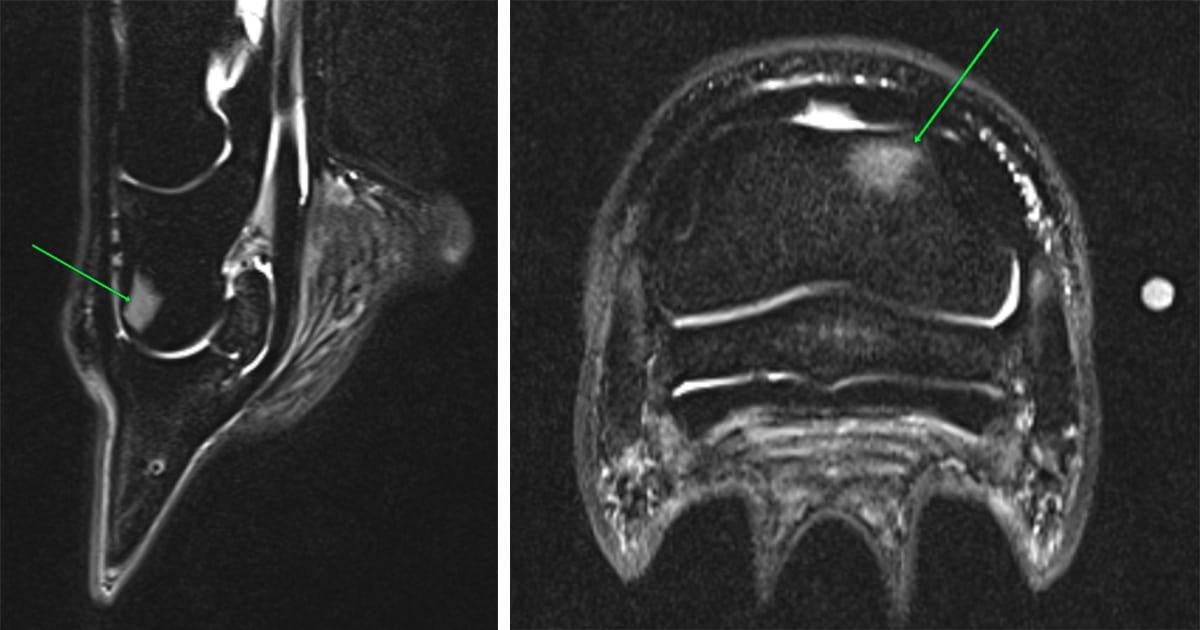
- Small (approximately 1 cm x 1.2 cm x 1.4 cm) focal region of moderate to marked fluid signal in the distal, dorsolateral second phalanx
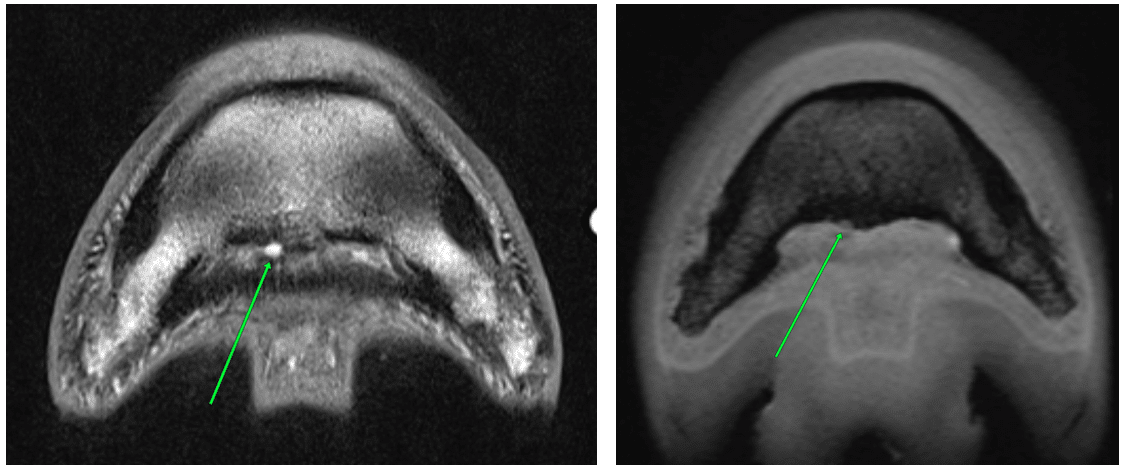
- Ill-defined PD and T1 hyperintensity along the dorsal aspect of the medial lobe of the deep digital flexor tendon at the proximal recess of the navicular bursa, continuing as a dorsally located focal region of hyperintensity and slight irregularity along the dorsal margin of the medial lobe at the level of the navicular bone
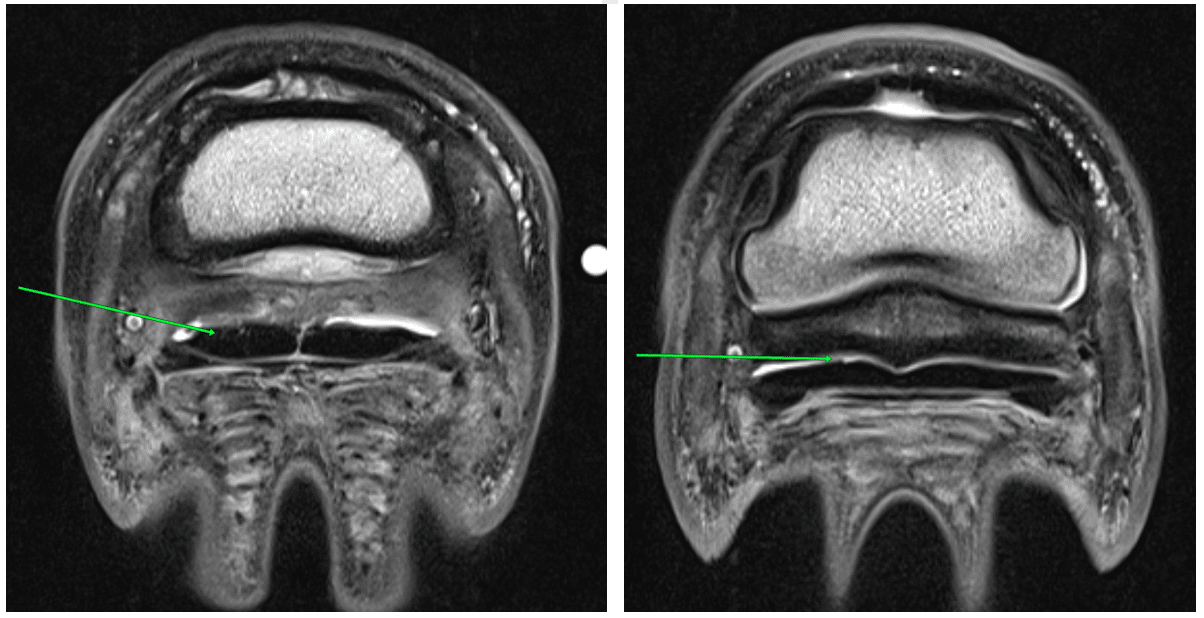
- Moderate navicular bursal effusion with moderate bursal wall thickening and intrabursal proliferative tissue
- Very small, focal region of mild hyperintensity in the deep digital flexor tendon medially at its insertion
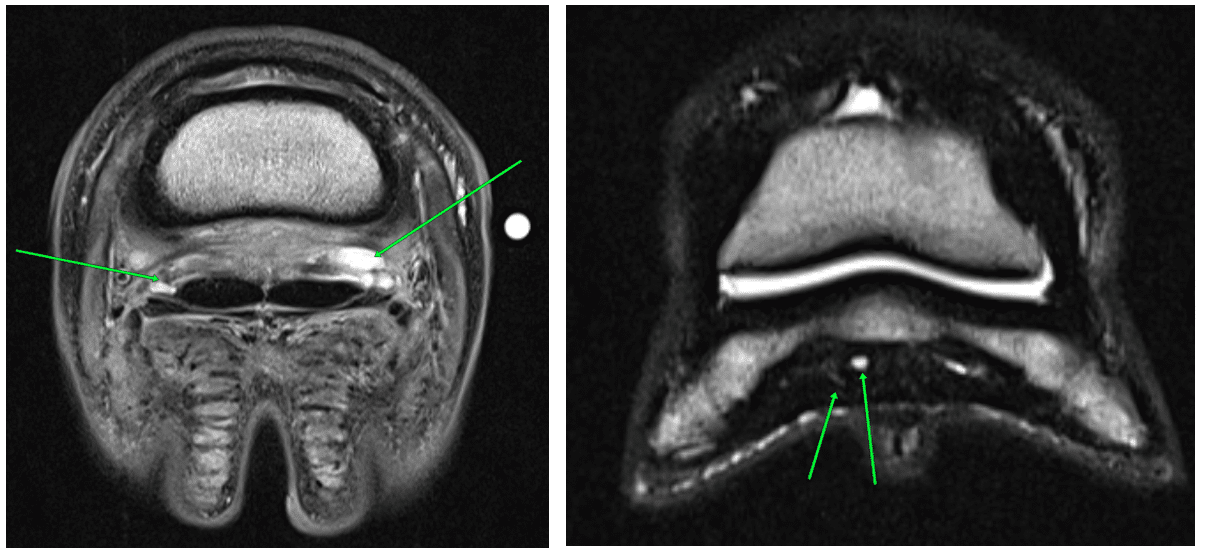
- Mild, ill-defined increased fluid signal in the palmar, central third phalanx near the impar ligament and deep digital flexor tendon insertions
- Focal rounded fluid accumulation between the deep digital flexor tendon and distal phalanx adjacent to the deep digital flexor insertion, medially, with mild adjacent osseous concavity/resorption; this likely represents fluid within the distal recess of the navicular bursa

Conclusions
- Moderate focal bone edema-like change in the distal, dorsolateral second phalanx. The primary differential is transient inflammation/contusion.
- Moderate proliferative navicular bursitis. Adhesion formation between the navicular bursa and the dorsal medial margin of the deep digital flexor tendon cannot be entirely excluded.
- Mild deep digital flexor tendinopathy, primarily affecting the dorsal margin of the medial lobe from the proximal recess of the navicular bursa to the navicular bone and minimally at the insertion.
- Mild bone edema-like change (degenerative change, inflammation) in the palmar, central third phalanx, supportive of chronic impar and/or deep digital flexor insertional enthesopathy.
- Focal fluid accumulation and minimal focal resorption along the palmar third phalanx immediately proximal to the deep digital flexor tendon insertion, likely within the distal recess of the navicular bursa and associated with chronic navicular bursitis.
- Mild navicular bone edema-like change. Differentials include mild/early degenerative change and/or transient inflammation.
- Mild bone edema-like change diffusely in the mid to distal aspect of the third phalanx. Differentials include degenerative change/fibrosis and/or transient inflammation/pedal osteitis.

Comments
The finding of primary clinical concern is the bone edema-like change in the distal, dorsolateral second phalanx. The changes in the navicular bursa and along the dorsal margin of the medial lobe of the deep digital flexor tendon likely contribute to the remainder of the patient’s lameness not alleviated with a lateral only abaxial nerve block. Further treatment/management recommendations may include longer rest/rehabilitation, bisphosphonate therapy (if not recently performed), and treatment of the navicular bursa.