
History
A nine year old, neutered male, labrador retriever with a history of 15 pound weight loss and intermittent GI upset was referred to Animal Imaging. On physical examination at our clinic, he was very nervous/anxious but alert and responsive. Mucous membranes were pink, CRT < 2 seconds, heart rate was elevated at 180 BPM with a grade 2/6 heart murmur PMI mitral. He was eupneic with normal lung sounds. No palpable neck masses were readily appreciated. No discrete, palpable thyroid mass on examination.
CBC/CHEM/UA/Thoracic Radiograph
His T4 levels were elevated at 7 (1-4 ug/dl) on the most recent blood work. The remainder of his CBC, chemistry panel and urinalysis are unremarkable. Thoracic radiographs were performed by the referring veterinarian and no abnormalities were identified. He was referred for thyroid scintigraphy by a local oncologist.
Thyroid Scintigraphy
He was sedated and thyroid scintigraphy was performed using 4 mCi of technetium. Images were obtained 20-30 minutes post injection of the radionuclide. Thyroid Scintigraphy
He was sedated and thyroid scintigraphy was performed using 4 mCi of technetium. Images were obtained 20-30 minutes post injection of the radionuclide.
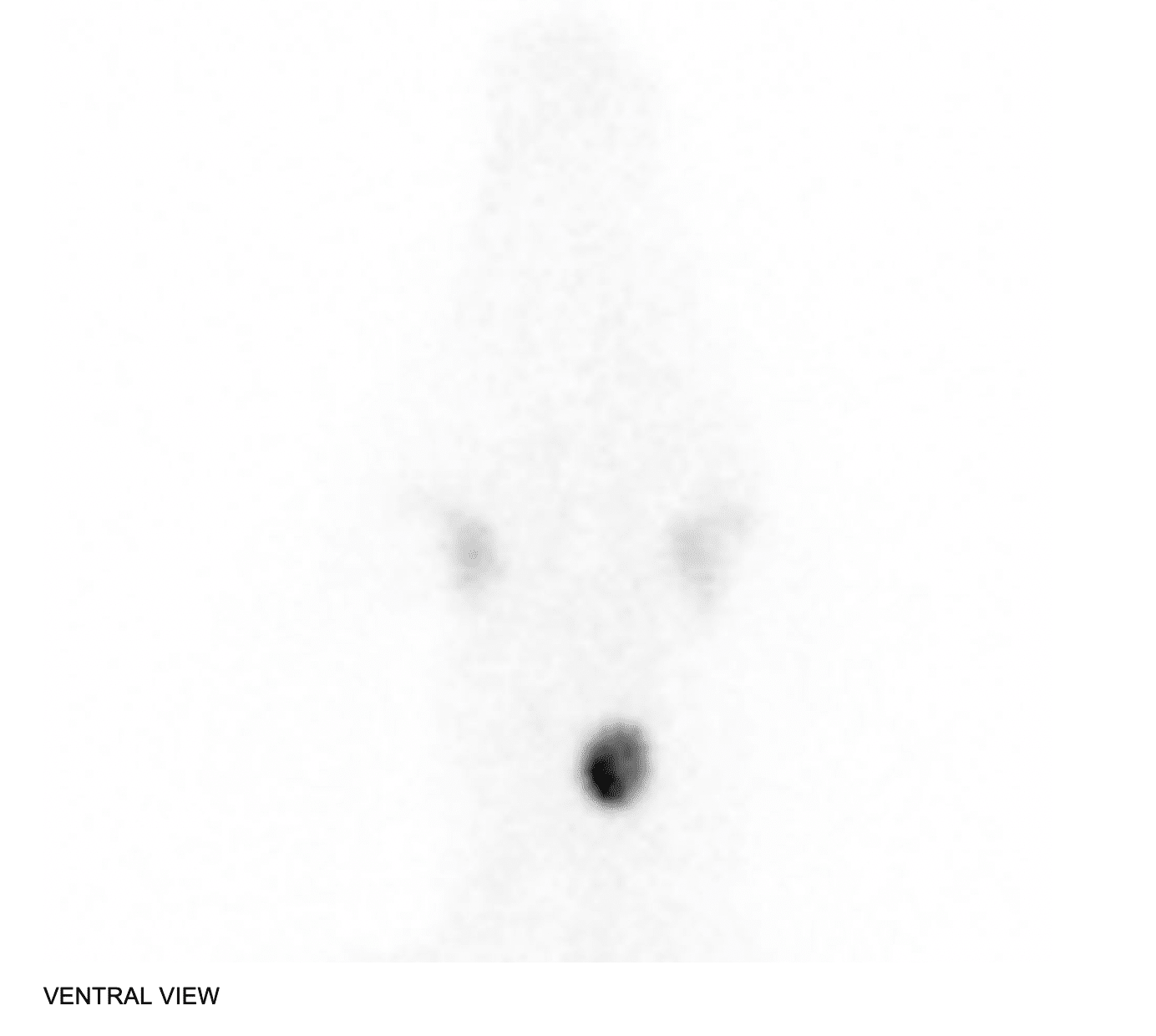
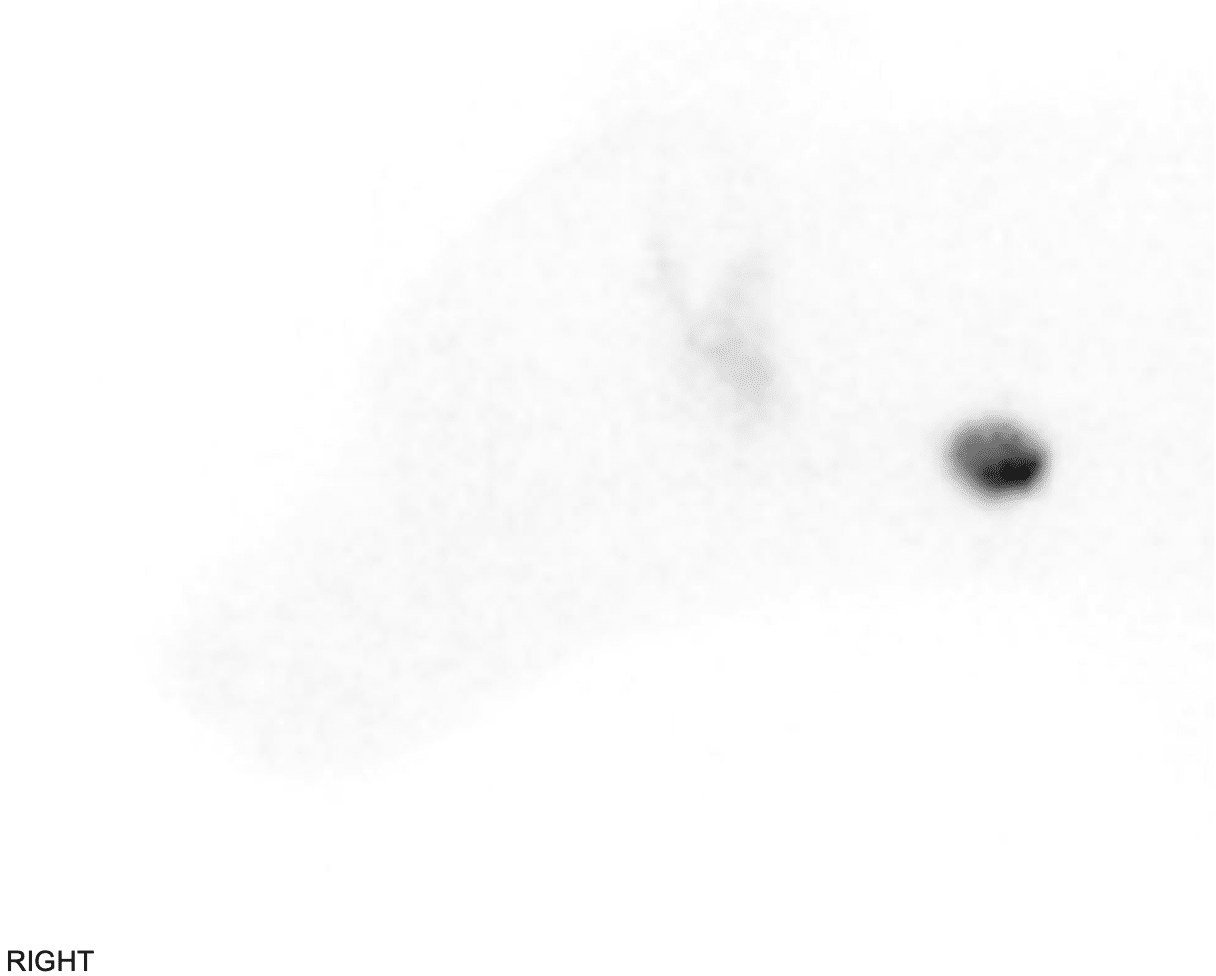
Scintigraphic findings:
A well-defined, rounded to oval region of increased radionuclide uptake is identified along the left aspect of the neck in the region of the left thyroid lobe. The pattern of uptake is mildly heterogeneous. Left thyroid to salivary gland ratio is elevated measuring approximately 4.5:1 (normal 1.12:1). There is complete suppression of the right thyroid lobe. No ectopic tissue is identified. No definitive abnormal foci of uptake are seen within the thorax.
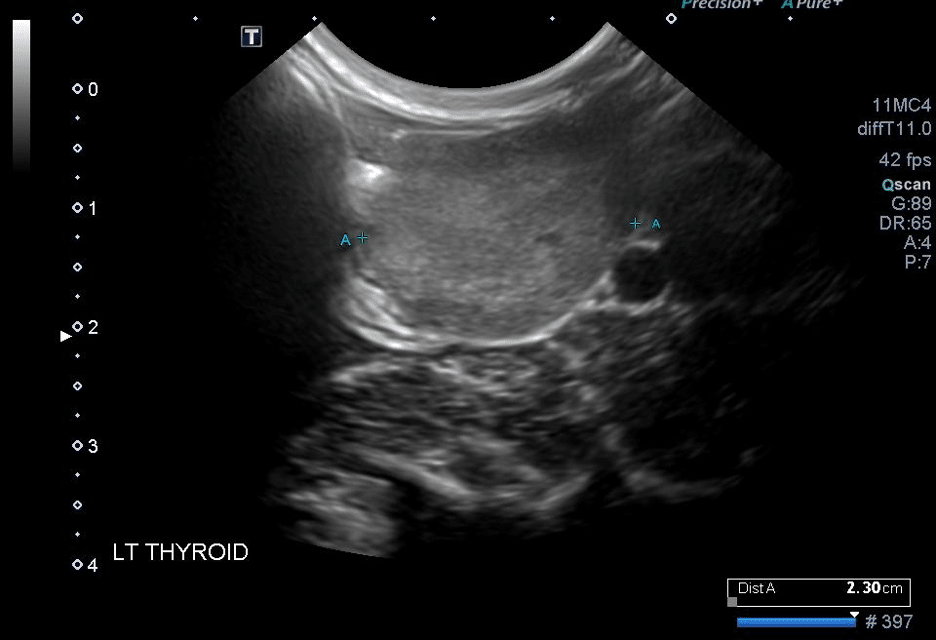
Limited/brief sonographic assessment of the thyroid lobes:
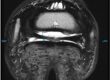
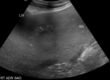
Left thyroid lobe: The left thyroid lobe is enlarged and oval in shape. It measures approximately 3.2 x 2.3 x 1.9 cm. (Normal being ~ 3.0 X 2.5 and 0.4-0.6cm in medium dogs).The left thyroid lobe is slightly heterogenous in appearance with amorphous hypoechoic regions along the dorsal aspects. The remainder of the gland is subtly mildly hyperechoic when compared to normal thyroidal tissue. The margins of the left thyroid lobe are well-defined. No definitive parathyroid glands are definitively identified. Right thyroid lobe: Not identified supporting complete suppression.

Conclusions:
He underwent a left thyroidectomy. Histopathology confirmed the diagnosis of thyroid follicular carcinoma with completely excised but narrowed margins. Thyroid carcinomas are uncommon but comprise approximately 90% of thyroid tumors in dogs. Approximately, 10% of thyroid carcinomas are functional. Ultrasound, CT and MRI are useful in determining the extent of soft tissue invasion for large, fixed tumors if surgical resection is planned or planning of radiation fields for radiation therapy. Nuclear scintigraphy is useful in determining function and identifying ectopic malignant tissue. Thyroid carcinomas are often metastatic at early stages of the disease, more frequently metastasizing to the lung. Ascending metastasis to the subcutaneous mandibular soft tissues has also been reported.